Both components of the sciatic nerve, common peroneal (CP) and tibial (T) nerves diverge from each other at the popliteal fossa. Lateral and medial gastrocne- mius muscles (GN) are also shown. The sural nerve is shown behind the lateral malleolus. .
Saphenous n
Blocks postero-medial part of dorsum of foot
Superficial infiltration around long saphenous vein anterosuperior to medial malleolus
Tibial n
Needle entry medial to Achilles tendon or lateral to posterior tibial artery at upper border of medial malleolus
Determine depth with paraesthesia, nerve stimulator or 1 cm superficial to tibia
Alternatively infiltration either side of artery behind medial malleolus
Blocks sole, plantar surface of digits
Deep peroneal n
Needle entry between extensor hallucis longus and tibialis anterior tendons or lateral to anterior tibial artery
Blocks first web space and short toe extensors
Superficial peroneal n
Superficial infiltration from lateral border of tibia to upper part of lateral malleolus
Blocks dorsum of foot and toes except first web space
Sural n
Superficial infiltration from Achilles tendon to lateral malleolus
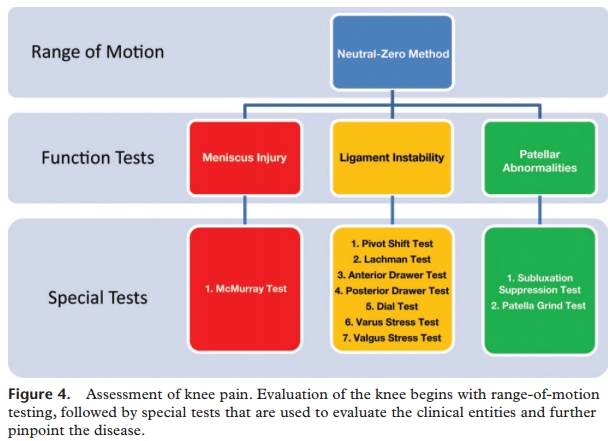
The physician begins by comparing the painful knee with the asymptomatic knee and inspecting the injured knee for erythema, swelling, bruising, and discoloration. The musculature should be symmetric bilaterally. The knee is then palpated and checked for pain, warmth, and effusion. Point tenderness should be sought, particularly at the patella, tibial tubercle, patellar tendon, quadriceps tendon, anterolateral and anteromedial joint line, medial joint line, and lateral joint line. LACHMAN TEST The Lachman test is another means of assessing the integrity of the anterior cruciate ligament (Figure 3).7 The test is performed with the patient in a supine position and the injured knee flexed to 30 degrees. The physician stabilizes the distal femur with one hand, grasps the proximal tibia in the other hand, and then attempts to sublux the tibia anteriorly. Lack of a clear end point indicates a positive Lachman test. ANTERIOR AND POSTERIOR DRAWER TEST VARUS AND VALGUS STRESS TEST The valgus stress test is performed with the patient's leg slightly abducted. The physician places one hand at the lateral aspect of the knee joint and the other hand at the medial aspect of the distal tibia. Next, valgus stress is applied to the knee at both zero degrees (full extension) and 30 degrees of flexion (Figure 4)7. With the knee at zero degrees (i.e., in full extension), the posterior cruciate ligament and the articulation of the femoral condyles with the tibial plateau should stabilize the knee; with the knee at 30 degrees of flexion, application of valgus stress assesses the laxity or integrity of the medial collateral ligament.








 .
.